Clinical Pathways for the 5 Wound Types
Choose a wound type to view the associated clinical pathways and guidelines.
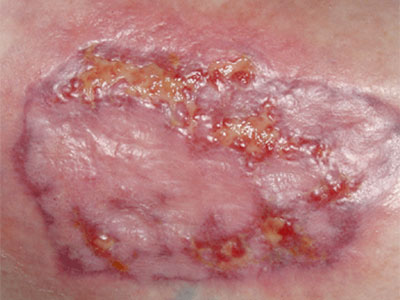
Diabetic Ulcer Pathway
 Refer to orthopaedic foot & ankle specialist or wound clinic
Refer to orthopaedic foot & ankle specialist or wound clinic - Goal of HgA1c < 8% to improve healing outcomes
- Evaluate for claudication, leg edema, and palpable foot pulses
- For non-palpable foot pulses, obtain vascular studies, refer to vascular surgery
- If this goes to bone, obtain x-rays of foot and refer to orthopaedic foot & ankle surgeon
- Start empiric broad-spectrum antibiotic (Augmentin, Clindamycin, Ciprofloxacin)
- Start wound care with saline moist gauze up to 2x/day depending on draining until infection resolves; then advanced dressing may be used to promote healing
- Refer to wound center

- Offloading is best obtained with a walking boot or cast
- Refer to orthotics for walking boot
- Refer to orthopaedics foot & ankle surgeon for cast
- Sharp debridement by specialists is usually the best approach
- Debridement can be done by primary care with the following therapies:
- Mechanical (cleansing, dressings)
- Enzymatic, (collagenase ointment)
- Autolytic (moisture retention dressings)
- Most wounds require all of the above to promote healing
- Referral to wound specialists can provide advanced dressing recommendations.
References
Glycemic control and post-operative healing. Journal of Foot and Ankle Research; Lower Extremity Review. Naohiro Shibuya, DPM, MS, FACFAS, Jon M. Humphers, DPM, and Daniel C. Jupiter, PhD. July 2013
>Guidelines for the treatment of diabetic ulcers; Wound Repair and Regeneration (2006). Wound Healing Society. Steed, David
Diagnosis and treatment of peripheral arterial disease in diabetic patients with a foot ulcer. A progress report of the International Working Group on the Diabetic Foot. Diabetic foot infection: Antibiotic guidelines. Johns Hopkins. Eric Nuermberger. 6/16/2009
Lipsky BA, Berendt AR, Deery HG, et al.; Diagnosis and treatment of diabetic foot infections.; Clin Infect Dis; 2004; Vol. 39; pp 885-910; ISSN: 1537-6591; PUBMED 15472838
Debridement: A Vital Component of Wound Bed Preparation. Kirshen C, Ayello E, Sibbald, R. Advances in Skin Wound Care 2006; 19:506-17; Lippincott Williams & Wilkins.